New Section!!!
*New " Case discussion " section
Loading
What is the pathophysiology of AS?
-
The stenosis that occurs at the aortic valve leads to pressure gradient from LV to aorta.To overcome this stenosis, the intracavitary increase in systolic pressure increases myocardial wall tension as stated by Laplace’s law
Wall tension = PR / 2h
-
This increase in wall tension is a direct stimulus or leads to parallel replication of sarcomere causing concentric hypertrophy.
-
The pressure gradient and the amount of cardiac output generated also is important as less pressure gradient may be generated when there is less cardiac output due to severe AS. This is explained by simplified Gorlin equation (Hakki equation)
AVA = CO / √ PG
Coronary perfusion
-
The increase in LVEDP causes decrease in coronary perfusion as CPP = ADP – LVEDP
-
Also, severe AS causes decrease in stroke volume which may compromise coronary perfusion.
-
Also, the coronary structural abnormalities, inadequate growth,increased systolic compression decrease the perfusion of hypertrophied myocardium.
Pressure Volume Loop
-
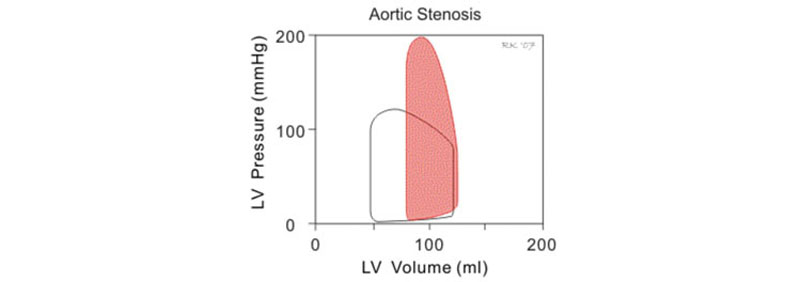
The PV loop in AS- main differences
-
Peak pressure generated during systole is much greater because of high pressure gradient
-
Slope of diastolic limb is steep because of decreased diastolic compliance due to LVH
-
This means small changes in diastolic in diastolic volume produce large increase in ventricular filling pressure
-
Systolic limb shows preservation of pump function (SV & EF)
Atrial kick
-
This increase in chamber stiffness makes “atrial kick” very important in AS.It contributes 40 % of LVEDV
-
Also, the isovolumic relaxation time is increased ( due to abnormal diastolic filling and ventricular relaxation) which leads to less filling during early rapid filling phase so atrial kick becomes so important
-
The “preload reserve” and LVH are compensatory mechanisms to maintain cardiac output when they fail, LV dilatation occurs and CHF ensues.
Prone for Ischaemia
The hypertrophied LV is more prone for ischaemia because of
-
Coronary abnormalities
-
Subendocardial ischaemia
-
Associated coronary artery disease
-
Decreased coronary perfusion pressure so decreased coronary supply
-
Increased MVO2
- by Dr Amarja
Viva Question List
© Copyright 2026 by Cardiacanaesthesia.in
CONTACT US • ABOUT US • DISCLAIMER • CONFERENCES 2026 •